Hyperprolactinemia and Infertility: A Fertility Specialist’s Experience
As a fertility specialist, I’ve encountered a range of causes for infertility, but one condition that often surprises women is hyperprolactinemia. It’s a condition where there’s too much prolactin in the blood—a hormone usually associated with breastfeeding. However, when prolactin levels are elevated outside of pregnancy or lactation, it can interfere with the delicate balance required for ovulation and conception.
I’ll never forget meeting Laura, a 32-year-old woman who came to me after a year of trying to conceive without success. She had regular cycles, no obvious issues with her partner’s sperm, and her health seemed otherwise fine. Yet, for some reason, pregnancy just wasn’t happening. We ran a series of tests, and what stood out was her elevated prolactin levels. This wasn’t something Laura expected. She wasn’t pregnant, wasn’t breastfeeding, and had no history of pituitary problems. But the lab results didn’t lie: her prolactin levels were too high. After some investigation, we discovered a small pituitary tumor (also called a prolactinoma) was the culprit.
Laura’s case taught me a lot about the often-overlooked role that prolactin plays in fertility, and how hyperprolactinemia can disrupt a woman’s ability to conceive.

What Is Hyperprolactinemia?
Hyperprolactinemia occurs when the body produces too much prolactin, the hormone that plays a key role in milk production after childbirth. In a normal reproductive cycle, prolactin levels rise and fall in response to signals from the brain and ovaries. However, when prolactin levels become too high—often due to a benign tumor in the pituitary gland—this delicate balance can be disrupted, leading to infertility.
Many women with hyperprolactinemia have no idea they have it, especially if they’re not experiencing the typical symptoms like galactorrhea (milk production unrelated to childbirth). This was the case with Laura, who was surprised when I explained that elevated prolactin levels could be interfering with her ability to ovulate.
Dr. Jane Miller, a reproductive endocrinologist I work closely with, says it best: “The link between prolactin and infertility isn’t always obvious. Most women with hyperprolactinemia don’t have the classic signs of milk production, so the condition can easily go undiagnosed until they’re struggling to conceive.”

How Hyperprolactinemia Affects Fertility
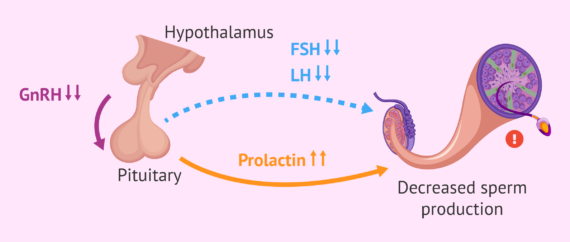
Prolactin is a hormone that’s crucial for pregnancy, but only after conception. Elevated prolactin levels can interfere with the hormonal signals that regulate ovulation. When prolactin is too high, it can prevent the release of the hormones FSH (follicle-stimulating hormone) and LH (luteinizing hormone), which are necessary for ovulation. Without regular ovulation, a woman’s chances of becoming pregnant decrease significantly.
The pituitary gland, located at the base of the brain, regulates prolactin production. When there’s a prolactinoma—a benign tumor on the pituitary—the gland produces excess prolactin, which suppresses ovulation. For women like Laura, the result is an anovulatory cycle, where eggs are not released from the ovaries, making natural conception extremely difficult.
I recall how Laura felt when we discussed her diagnosis. At first, she was shocked. “How could something as simple as a hormone imbalance keep me from having a baby?” she asked. It’s a question I hear often in my practice, and it speaks to how invisible hormonal imbalances can be, until they disrupt the body’s ability to function normally.

Diagnosing Hyperprolactinemia
The first step in diagnosing hyperprolactinemia is through a simple blood test that measures prolactin levels. If the levels are higher than normal, further testing is needed to identify the cause. In most cases, the cause is a benign pituitary tumor, known as a prolactinoma.
In Laura’s case, after confirming her elevated prolactin levels, we conducted an MRI, which revealed a small prolactinoma on her pituitary gland. While most prolactinomas are benign and slow-growing, they can cause significant hormonal imbalances, and in some cases, they can be large enough to press on surrounding brain tissue, leading to vision changes or headaches.
It’s crucial to rule out other causes of elevated prolactin, such as thyroid disorders, kidney disease, or medications that affect prolactin levels (such as antipsychotic drugs). Once a diagnosis is made, treatment can begin.
Dr. Mark Collins, a renowned endocrinologist, once said, “Prolactinomas are very common and often go undetected, which is why it’s important for fertility specialists to consider elevated prolactin levels in women who aren’t ovulating, even if they don’t have symptoms like galactorrhea.”
Treatment Options for Hyperprolactinemia-Related Infertility
The good news for women like Laura is that hyperprolactinemia can be treated, and fertility can often be restored. Treatment depends on the underlying cause and the severity of the prolactin elevation. Here are the most common treatment options:
- Medications (Dopamine Agonists)
The most common treatment for hyperprolactinemia is the use of dopamine agonists, such as cabergoline or bromocriptine. These medications work by reducing prolactin production and shrinking the prolactinoma, if present. In most cases, these medications help restore normal ovulation and improve the chances of conception.Laura was prescribed cabergoline, and within a few months, her prolactin levels returned to normal. Her periods became regular again, and her chances of conceiving improved significantly.
- Surgery
If the prolactinoma is large or resistant to medication, surgery may be required. However, surgery is rarely necessary, as dopamine agonists are usually very effective in controlling prolactin levels. - IVF
In some cases, if medication and other treatments do not result in conception, IVF (in vitro fertilization) can be considered. This is especially the case for women who have been dealing with elevated prolactin levels for a long time, as the condition may cause irreversible damage to the ovaries or other reproductive structures.
Laura’s Journey to Pregnancy
Laura’s story is one that brings me joy to tell. After a few months of taking cabergoline, her prolactin levels normalized, and she began ovulating again. Six months later, we saw the good news: Laura was pregnant. She went on to have a healthy baby girl, and the joy and relief she felt were indescribable.
As I spoke to her during her pregnancy, she told me how much she had learned from her experience. “I had no idea that a small hormone imbalance could make such a big difference,” she said. “I’m just grateful we figured it out and found a solution.”
Dr. Emily Lewis, one of my colleagues in the fertility clinic, often says, “Hyperprolactinemia is one of those conditions that many women don’t know about until they encounter infertility, but the good news is that with the right treatment, the vast majority of women can conceive.”
Conclusion: There’s Hope for Those Struggling with Hyperprolactinemia
If you’re struggling to conceive and have been diagnosed with hyperprolactinemia, I want you to know that there’s hope. With the right treatment, such as dopamine agonists, many women go on to have successful pregnancies. Whether the cause is a small prolactinoma or another issue, fertility can often be restored, and with it, the chance to build the family you’ve been dreaming of.
As a fertility specialist, it’s a privilege to walk alongside women like Laura as they navigate the journey to motherhood. If you’re dealing with hyperprolactinemia and infertility, don’t lose hope—there are solutions, and with the right care, you too can become a mother.
If you’re experiencing similar health issues, please feel free to contact us. Our team is here to offer expert advice and personalized care. We are happy to answer your questions and discuss potential treatment options.



{kind=link}
No comment